Managing intestinal failure–associated liver disease (IFALD) requires a two-pronged approach by specialty pharmacists: keeping an eye on the orphan drug pipeline for IFALD, and tracking potential causes of the disorder, including total parental nutrition (TPN), according to several experts.
The relationship between TPN and IFALD warrants the attention of clinicians who manage vulnerable patients, stressed Kathleen Gura, PharmD, the board director at the American Society for Parenteral and Enteral Nutrition, whose research focuses on IFALD.
In the 40 years Dr. Gura has been studying IFALD, academic centers identified many potential contributing factors to the disease’s development, including the microbiome and the oil content of the IV fat emulsions. Physicians created nutritional strategies that allow these vulnerable patients to improve. Over time, they can even come off TPN entirely.

“When you look at how we care for these children, we are doing much better than 20 to 25 years ago,” said Valeria Cohran, MD, the director of intestinal rehabilitation at The Ann & Robert H. Lurie Children’s Hospital, in Chicago. However, the evidence on the nutritional strategies used in this patient group remains scant. It’s a small, heterogeneous group and each patient’s treatment varies based on their unique intestinal anatomy. Furthermore, in her four decades working in intestinal rehabilitation, Laura Matarese, RDN, a researcher and dietitian at ECU Health, in Greenville, N.C., said she had never had any two patients who were exactly alike.
In addition, liver biopsies are nearly impossible to safely perform in infants, according to Dr. Gura. “It’s very, very dangerous; they could potentially bleed to death,” she said. With no one-size-fits-all approach, physician, pharmacist and dietitian experts discussed how they interpret and apply the available data on IFALD nutrition.
Ensuring Patients Get Essential Nutrients
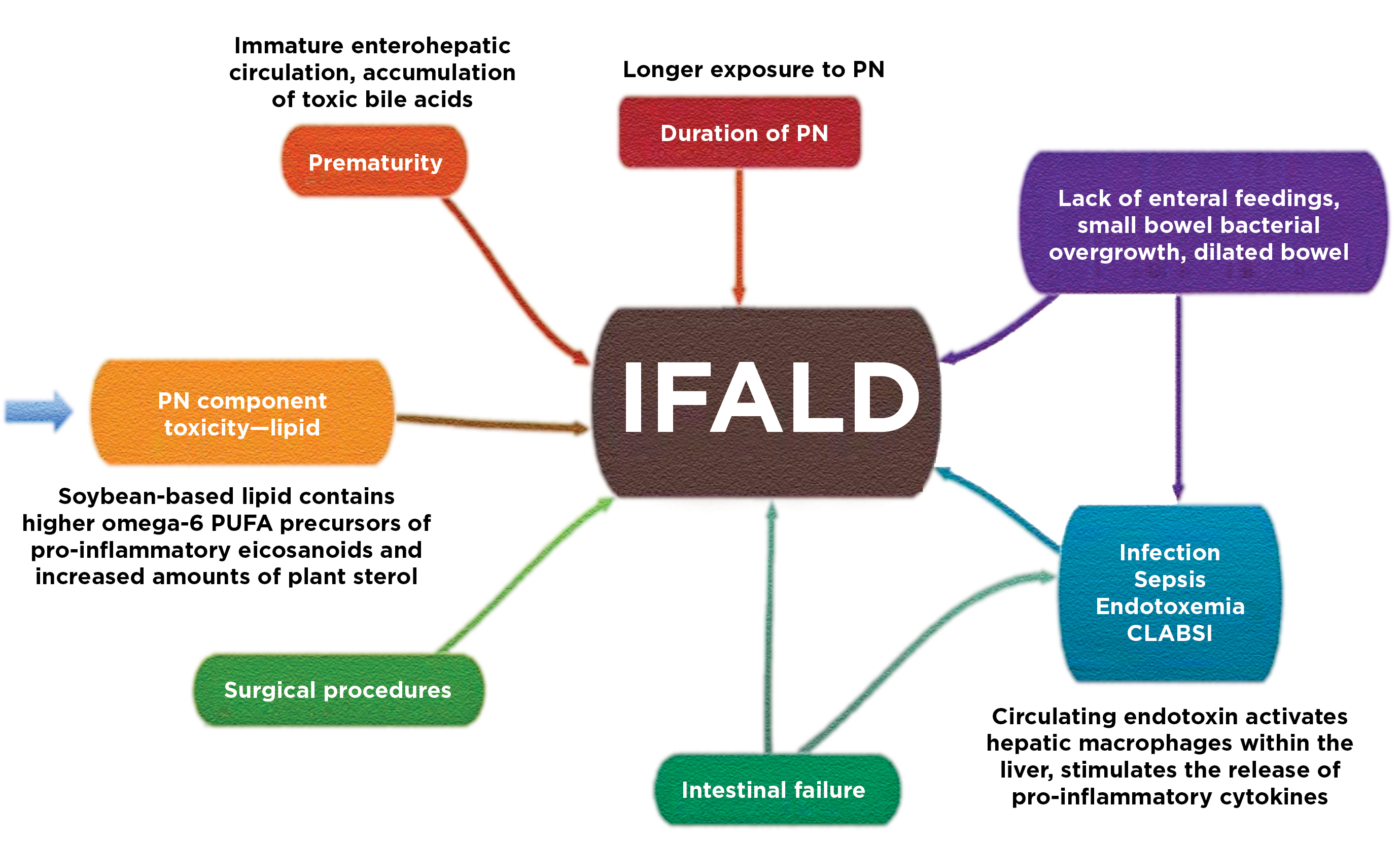
The challenge lies in ensuring patients have essential nutrients, and children get enough nutrition to grow, while avoiding toxicity. IFALD is characterized by progressive cholestasis and biliary fibrosis, and steatohepatitis in adults, after prolonged TPN (Hepatol Int 2020;14[3]:305-316). Although TPN is necessary, it’s a high-risk therapy, Dr. Gura said. Overfeeding dextrose and lipids by IV can injure the liver, she noted. Moreover, the IV catheter required to deliver nutrients puts patients at risk for infection and sepsis, which also can contribute to liver injury.
These risks (Figure) exist for anyone on TPN, but for young children—premature infants especially—their immature livers can’t withstand much to begin with. So, they are “less able to tolerate [TPN] than an adult or older child,” Dr. Cohran said. Jaundice and liver injury often don’t show up in adults until the disease has progressed much further, according to Dr. Gura. In contrast, infants can start to show symptoms within three weeks of starting TPN, she said.
One of the reasons that care for IFALD patients has improved so dramatically since the early 2000s is a better understanding of how different IV lipid emulsions affect patients. For decades after the emulsions were introduced in the United States in the 1970s, no one suspected they contributed to IFALD, Dr. Gura said. That’s because patients appeared to develop IFALD with lipid emulsions and without them.
In the early 2000s, it became clear that liver disease was happening by two different mechanisms, she said. Without fat, patients would develop steatosis due to de novo lipogenesis. However, patients receiving high doses of soybean oil lipid emulsions also ended up with liver disease because the emulsion can be hepatotoxic.
Soybean oil emulsions are actually a very good source of essential fatty acids even when given at a low dose, Dr. Gura said. But physicians and researchers hypothesize that the emulsion lacks sufficient alpha-tocopherol or contains too many phytosterols that infants can’t properly metabolize. It’s also possible that excessive inflammatory omega-6 fatty acids in soybean oil emulsions and reduced amount of omega-3 fatty acids may prevent hepatocytes from resisting oxidative stress, according to an FDA webinar in May 2022.
“There’s no prospective data that composite lipids”—a mixture of oil emulsions such as SMOFlipid (Fresenius Kabi), an injectable emulsion, rather than just soybean oil alone—“is different, but that’s the conventional thought,” Dr. Cohran said.
In 2013, the FDA mandated postmarketing safety studies of Nutralipid, a 20% soybean oil IV fat emulsion (B. Braun); Intralipid, an IV emulsion of soybean oil (Baxter/Fresenius Kabi); and Clinolipid, a 20% lipid injectable emulsion (Baxter). The agency called for the studies based on new data that implicated phytosterols, found in abundance in soybean oil–containing emulsions, in IFALD.
According to the FDA, phytosterols are largely unabsorbed in the gastrointestinal tract and even prevent the absorption of cholesterol. However, when infused, phytosterols can accumulate and decrease bile acid synthesis. This in turn increases the phytosterol content in bile, which can lead to cell lysis and damage hepatocytes. That damage is compounded by common conditions in neonates such as gut resection, sepsis and immaturity, according to an FDA webinar (bit.ly/3A4RWqu) presentation by Camelia Martin, MD, the chief of newborn medicine at Weill Cornell Medicine, in New York City.
A study in pigs, published in the Journal of Parenteral and Enteral Nutrition in March 2022, found normal phytosterol concentrations (such as that in Intralipid 100% soybean oil) and enriched phytosterol concentrations caused higher direct bilirubin concentrations than emulsions with depleted phytosterol content (JPEN J Parenter Enteral Nutr 2022;46[1]:160-171).

A study of neonates by Fresenius Kabi found those receiving the company’s low-phytosterol lipid emulsion, SMOFlipid, were less likely to develop parenteral nutrition–associated cholestasis (2/83; 2.4%), which is a precursor to IFALD, than those receiving a 100% soybean oil emulsion (9/78; 11.5%). Most cases of parenteral nutrition–associated liver disease (PNALD) occurred after 28 days, suggesting long-term use was a significant contributor (ClinicalTrials.gov Identifier: NCT02579265).
In a 2020 study of neonates diagnosed with IFALD, switching to 100% fish oil (Omegaven, Fresenius Kabi) reversed the liver disease in 11 of 15 infants (J Clin Med 2020;9[11]:3393).
However, a meta-analysis from 2016 did not find fish oil containing SMOFlipid to have a strong protective effect against IFALD compared with 100% soybean oil, despite a sevenfold reduction in phytosterols (J Pediatr Gastroenterol Nutr 2016;62[5]:776-792). Similarly, a Cochrane Review did not find any lipid emulsions with or without fish oil to provide better protection against PNALD (Cochrane Database Syst Rev 2019;6:CD013163).
Finding the Best Lipid Profile Not Easy
Even with a better understanding of the limitations of soybean oil, the choice of lipid emulsion for patients coming into the neonatal ICU isn’t always straightforward. Drs. Cohran and Gura said they continue to use soybean oil for their patients. Dr. Cohran prefers a composite lipid emulsion, one made of multiple lipid types such as soybean oil, olive oil, MCT (or medium-chain triglycerides) oil and fish oil. She uses soybean oil in low amounts and carefully monitors total and direct bilirubin. When bilirubin reaches 2 mg/dL, an indication of IFALD, she switches patients to Omegaven.
Dr. Gura said each lipid source has its limitations and its place in treating unique patient cases. A soybean oil such as Nutralipid or Intralipid has a long history of use, is efficient in terms of required fatty acids and is well tolerated for a short duration of therapy, she noted.
Investigational Agents
Several drugs are in development for IFALD, with their sponsors seeking orphan drug status for the agents. One such drug, IV Choline Chloride, a substrate replacement for IFALD patients, is being developed by Artara Therapeutics. In a phase 2 study, the drug met its objective of reversing steatosis and improving cholestasis as compared with placebo (bwnews.pr/3hb5JV3).
Beyond lipids and investigational agents, experts said prioritizing enteral nutrition in neonates and oral feeding in adults is crucial. In infants, feeding enterally helps the remaining intestine adapt and improves the likelihood they can transition from TPN entirely. “With [adult] oral intake, the liver gets first pass at those nutrients,” Ms. Matarese said. In contrast, with TPN, the liver typically is last for nutrient delivery.
Oral feeding in adults also stimulates enteral hepatic circulation, villus height and crypt depth, she said. “If there is any way I can rehabilitate the remnant bowel, I think it offers the best potential for health and improved quality of life,” Ms. Matarese stressed.
Team Effort Best for Care
Adding pharmacists and dietitians to the nutrition team can help ensure patients are receiving the appropriate formula based on their intestinal anatomy. The pharmacists and dietitians can check, for example, if patients are receiving the appropriate vitamins and minerals, especially in the current time of shortages, and that enteral nutrition is formulated for a patient’s unique anatomy and limitations. If a patient lacks their distal small bowel, they’re likely to have a vitamin B12 deficiency and also absorb fat-soluble vitamins poorly, Dr. Cohran said. If patients are missing their proximal small intestine, they are more susceptible to iron deficiency.
Specialized Centers
Pharmacists and dietitians also can help access products and reconcile TPN recipes, Dr. Cohran said. This collaboration is likely to be one reason that patients who receive treatment at a specialized center have better outcomes. There’s a bigger opportunity for out-of-the-box and holistic thinking with a multidisciplinary team, Dr. Gura said. Dr. Cohran has patients who travel more than five hours to be seen by her team in Chicago.
But “everybody can’t jump on a plane to fly to Boston, Cincinnati or Chicago,” Dr. Cohran said. If a provider is trying to support a patient who has IFALD but is not located near a major center, getting in touch with a large center can be critical, Dr. Gura said, as is diving into the rapidly evolving literature on IFALD. It may be useful to ask nearby professionals such as pharmacists, dietitians, social workers or neonatologists to help. At first, a gastroenterologist may need to mentor a pharmacist because most don’t receive formal training in this area, Dr. Gura said. However, it will become a very useful partnership quickly, she said.
All three experts said there is a way to see patients return to a more normal life, to see children safe to swim and rough-house with their siblings, Dr. Cohran said. “What drives me is tapering children from TPN and allowing them to live their best life.”
Dr. Cohran reported financial relationships with Abbott Nutrition, Nutricia and Takeda. Dr. Gura reported financial relationships with Alcresta, Fresenius Kabi, Lexicomp, NorthSea Therapeutics and Otsuka Pharmaceutical Factory. Dr. Matarese reported no relevant financial disclosures.
{RELATED-HORIZONTAL}